



| Carpal tunnel syndrome | |
|---|---|
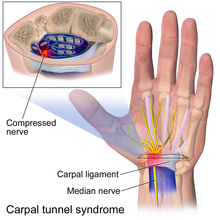
Transverse section at the wrist.
The median nerve is colored yellow.
The carpal tunnel consists of the bones and transverse carpal ligament.
|

People with CTS experience numbness, tingling, or burning sensations in the thumb and fingers, in particular the index and middle fingers and radial half of the ring finger, because these receive their sensory and motor function (muscle control) from the median nerve. Less-specific symptoms may include pain in the wrists or hands, loss of grip strength, and loss of manual dexterity.
Numbness and paresthesias in the median nerve distribution are the hallmark neuropathic symptoms (NS) of carpal tunnel entrapment syndrome. Weakness and atrophy of the thumb muscles may occur if the condition remains untreated, because the muscles are not receiving sufficient nerve stimulation. Discomfort is usually worse at night and in the morning.
Most cases of CTS are of unknown cause. Carpal tunnel syndrome can be associated with any condition that causes pressure on the median nerve at the wrist. Some common conditions that can lead to CTS include obesity, oral contraceptives, hypothyroidism, arthritis, diabetes, prediabetes (impaired glucose tolerance), and trauma. Carpal tunnel is also a feature of a form of Charcot-Marie-Tooth syndrome type 1 called hereditary neuropathy with liability to pressure palsies.
Other causes of this condition include intrinsic factors that exert pressure within the tunnel, and extrinsic factors (pressure exerted from outside the tunnel), which include benign tumors such as lipomas, ganglion, and vascular malformation. Carpal tunnel syndrome often is a symptom of transthyretin amyloidosis-associated polyneuropathy and prior carpal tunnel syndrome surgery is very common in individuals who later present with transthyretin amyloid-associated cardiomyopathy, suggesting that transthyretin amyloid deposition may cause carpal tunnel syndrome.
The median nerve can usually move up to 9.6 mm to allow the wrist to flex, and to a lesser extent during extension. Long-term compression of the median nerve can inhibit nerve gliding, which may lead to injury and scarring. When scarring occurs, the nerve will adhere to the tissue around it and become locked into a fixed position, so that less movement is apparent.
Normal pressure of the carpal tunnel has been defined as a range of 2–10 mm, and wrist flexion increases this pressure 8-fold, while extension increases it 10-fold. Repetitive flexion and extension in the wrist significantly increase the fluid pressure in the tunnel through thickening of the synovial tissue that lines the tendons within the carpal tunnel.
The international debate regarding the relationship between CTS and repetitive motion in work is ongoing. The Occupational Safety and Health Administration (OSHA) has adopted rules and regulations regarding cumulative trauma disorders. Occupational risk factors of repetitive tasks, force, posture, and vibration have been cited. The relationship between work and CTS is controversial; in many locations, workers diagnosed with carpal tunnel syndrome are entitled to time off and compensation.
Some speculate that carpal tunnel syndrome is provoked by repetitive movement and manipulating activities and that the exposure can be cumulative. It has also been stated that symptoms are commonly exacerbated by forceful and repetitive use of the hand and wrists in industrial occupations, but it is unclear as to whether this refers to pain (which may not be due to carpal tunnel syndrome) or the more typical numbness symptoms.
A variety of patient factors can lead to CTS, including heredity, size of the carpal tunnel, associated local and systematic diseases, and certain habits. Non-traumatic causes generally happen over a period of time, and are not triggered by one certain event. Many of these factors are manifestations of physiologic aging.
Examples include:
Numbness in the distribution of the median nerve, nocturnal symptoms, thenar muscle weakness/atrophy, positive Tinel's sign at the carpal tunnel, and abnormal sensory testing such as two-point discrimination have been standardized as clinical diagnostic criteria by consensus panels of experts. Pain may also be a presenting symptom, although less common than sensory disturbances.
Electrodiagnostic testing (electromyography and nerve conduction velocity) can objectively verify the median nerve dysfunction. Normal nerve conduction studies, however, do not exclude the diagnosis of CTS. Clinical assessment by history taking and physical examination can support a diagnosis of CTS. If clinical suspicion of CTS is high, treatment should be initiated despite normal electrodiagnostic testing.
The use of Phalen test, Tinel sign, Flick sign, or upper limb nerve test alone is not sufficient for diagnosis.
Other conditions may also be misdiagnosed as carpal tunnel syndrome. Thus, if history and physical examination suggest CTS, patients will sometimes be tested electrodiagnostically with nerve conduction studies and electromyography. The goal of electrodiagnostic testing is to compare the speed of conduction in the median nerve with conduction in other nerves supplying the hand. When the median nerve is compressed, as in CTS, it will conduct more slowly than normal and more slowly than other nerves.

Suggested healthy habits such as avoiding repetitive stress, work modification through use of ergonomic equipment (wrist rest, mouse pad), taking proper breaks, using keyboard alternatives (digital pen, voice recognition, and dictation), and have been proposed as methods to help prevent carpal tunnel syndrome.
Stretches and isometric exercises will aid in prevention for persons at risk. Stretching before the activity and during breaks will aid in alleviating tension at the wrist. Place the hand firmly on a flat surface and gently pressing for a few seconds to stretch the wrist and fingers. An example for an isometric exercise of the wrist is done by clenching the fist tightly, releasing and fanning out fingers. None of these stretches or exercises should cause pain or discomfort.
Biological factors such as genetic predisposition and anthropometric features had significantly stronger causal association with carpal tunnel syndrome than occupational/environmental factors such as repetitive hand use and stressful manual work. This suggests that carpal tunnel syndrome might not be preventable simply by avoiding certain activities or types of work/activities.
Generally accepted treatments include:
The American Academy of Orthopedic Surgeons recommends proceeding conservatively with a course of nonsurgical therapies tried before release surgery is considered. A different treatment should be tried if the current treatment fails to resolve the symptoms within 2 to 7 weeks. Early surgery with carpal tunnel release is indicated where there is evidence of median nerve denervation or a person elects to proceed directly to surgical treatment. Recommendations may differ when carpal tunnel syndrome is found in association with the following conditions: diabetes mellitus, coexistent cervical radiculopathy, hypothyroidism, polyneuropathy, pregnancy, rheumatoid arthritis, and carpal tunnel syndrome in the workplace.


The importance of wrist braces and splints in the carpal tunnel syndrome therapy is known, but many people are unwilling to use braces. Current recommendations generally don't suggest immobilizing braces, but instead activity modification and non-steroidal anti-inflammatory drugsas initial therapy, followed by more aggressive options or specialist referral if symptoms do not improve.
Many health professionals suggest that, for the best results, one should wear braces at night and, if possible, during the activity primarily causing stress on the wrists.
Corticosteroid injections can be effective for temporary relief from symptoms while a person develops a long-term strategy that fits their lifestyle. The injections are done under local anæsthesia. This treatment is not appropriate for extended periods, however. In general, local steroid injections are only used until other treatment options can be identified.

Release of the transverse carpal ligament is known as "carpal tunnel release" surgery. It is recommended when there is static (constant, not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting or other conservative interventions no longer control intermittent symptoms. The surgery may be done with local or regional anesthesia with or without sedation, or under general anesthesia. In general, milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment.
Surgery is more beneficial in the short term to alleviate symptoms (up to six months) than wearing an orthosis for a minimum of 6 weeks. However, surgery and wearing a brace resulted in similar symptom relief in the long term (12-18 month outcomes).
A recent evidence based guideline produced by the American Academy of Orthopedic Surgeons assigned various grades of recommendation to physiotherapy (also called physical therapy) and other nonsurgical treatments. One of the primary issues with physiotherapy is that it attempts to reverse (often) years of pathology inside the carpal tunnel. Practitioners caution that any physiotherapy such as myofascial release may take weeks of persistent application to effectively manage carpal tunnel syndrome.
Again, some claim that pro-active ways to reduce stress on the wrists, which alleviates wrist pain and strain, involve adopting a more ergonomic work and life environment. For example, some have claimed that switching from a QWERTY computer keyboard layout to a more optimised ergonomic layout such as Dvorak was commonly cited as beneficial in early CTS studies, however some meta-analyses of these studies claim that the evidence that they present is limited.

Most people relieved of their carpal tunnel symptoms with conservative or surgical management find minimal residual or "nerve damage". Long-term chronic carpal tunnel syndrome (typically seen in the elderly) can result in permanent "nerve damage", i.e. irreversible numbness, muscle wasting, and weakness. Those that undergo a carpal tunnel release are nearly twice as likely as those not having surgery to develop trigger thumb in the months following the procedure.
While outcomes are generally good, certain factors can contribute to poorer results that have little to do with nerves, anatomy, or surgery type. One study showed that mental status parameters or alcohol use yields much poorer overall results of treatment.
Recurrence of carpal tunnel syndrome after successful surgery is rare. If a person has hand pain after surgery, it is most likely not caused by carpal tunnel syndrome. It may be the case that the illness of a person with hand pain after carpal tunnel release was diagnosed incorrectly, such that the carpal tunnel release has had no positive effect upon the patient's symptoms.
Carpal tunnel syndrome can affect anyone. It accounts for about 90% of all nerve compression syndromes. In the U.S., 5% of people have the effects of carpal tunnel syndrome. Caucasians have the highest risk of CTS compared with other races such as non-white South Africans. Women suffer more from CTS than men with a ratio of 3:1 between the ages of 45–60 years. Only 10% of reported cases of CTS are younger than 30 years. Increasing age is a risk factor. CTS is also common in pregnancy.
|
Page Content |
