



| Spondylolysis | |
|---|---|

Spondylolysis
|
Spondylolysis is a bony defect or fracture within the pars interarticularis of the vertebral arch in the spinal column. The vast majority of spondylolysis occur in the lumbar vertebrae, however it can also be seen in cervical vertebrae. The lumbar vertebra consist of a body, pedicle, lamina, pars interarticularis, transverse process, spinous processand superior and inferior articular facets, which form joints that link the vertebrae together. When examining the vertebra, the pars interarticularis is the bony segment between the superior and inferior articular facet joints located anterior to the lamina and posterior to the pedicle. Separation of the pars interarticularis occurs when spondylolysis is present in the spinal column.
Spondylolysis is typically caused by a stress fracture of the bone, and is especially common in adolescents who over-train in activities. The pars interarticularis is vulnerable to fracture during spinal hyperextension, especially when combined with rotation, or when experiencing a force during a landing. This stress fracture most commonly occurs where the concave lumbar spine transitions to the convex sacrum (L5-S1). A significant amount of individuals with spondylolysis will develop spondylolisthesis, which is true for 50-81% of this population.
The cause of spondylolysis remains unknown, however many factors are thought to contribute to its development. The condition is present in up to 6% of the population, majority of which usually present asymptomatically. Research supports that there are hereditary and acquired risk factors that can make one more susceptible to the defect. The disorder is generally more prevalent in males compared to females, and tends to occur earlier in males due to their involvement in more strenuous activities at a younger age. In a young athlete, the spine is still growing which means there are many ossification centers, leaving points of weakness in the spine. This leaves young athletes at increased risk, particularly when involved in repetitive hyperextension and rotation across the lumbar spine. Spondylolysis is a common cause of low back in preadolescents and adolescent athletes, as it accounts for about 50% of all low back pain. It is believed that both repetitive trauma and an inherent genetic weakness can make an individual more susceptible to spondylolysis.
In majority of cases, spondylolysis presents asymptomatically which can make diagnosis both difficult and incidental. When a patient does present with symptoms, there are general signs and symptoms a clinician will look for:
Sports involving repetitive or forceful hyperextension of the spine, especially when combined with rotation are the main mechanism of injury for spondylolysis. The stress fracture of the pars interarticularis occurs on the side opposite to activity. For instance, for a right handed player, the fracture occurs on the left side of the vertebrae.
Spondylolysis has a higher occurrence in the following activities:
Although this condition can be caused by repetitive trauma to the lumbar spine in strenuous sports, however other risk factors can predispose individuals to spondylolsis. Males are more commonly affected by spondylolysis than females. In one study looking at youth athletes, it was found that the mean age of individuals with spondylolisthesis wasis 20 years of age. Spondylolysis also runs in families suggesting a hereditary component such as a predisposition to weaker vertebrae.
There are several imaging techniques used to diagnose spondylolysis. Common imaging techniques include X-ray, MRI, Bone Scintigraphy (Bone Scan), and Computed Tomography (CT Scan). Qualified health care practitioners are also able to conduct clinical tests such as the one-legged hyperextension test to diagnose active spondylolysis.
This is a test conducted by a qualified healthcare practitioner within a clinical setting. It involves having the patient stand upon one leg and then lean backwards. The test should produce pain on the same side of the spine as the leg that you are standing on. If it produces pain this indicates spondylolysis on that side. The test is then performed on the other side assessing for pain again. The test can be positive on one side, both sides or neither.
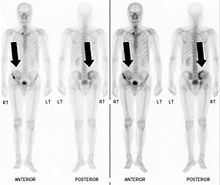
Also known as a bone scan, bone scintigraphy involves the injection of a small amount of radioactive tracer into the bloodstream. This tracer decays and emits radioactive energy which can be detected by a special camera. The camera produces a black and white image where areas shown as dark black indicate bone damage of some kind. If there is a black spot in the lumbar vertebrae (e.g. L5) this indicates damage and potentially spondylolysis. If this test is positive, a CT scan is usually ordered to confirm spondylolysis.
X-ray imaging uses electromagnetic radiation and projects it into the body. The radiation is blocked by the dense tissues of the body (i.e. bone) and appear white on the image that is produced. Tissues that contain air and are less dense appear as black on the x-ray image. A vertebra with a fracture will have a black mark in it. The black mark will appear on the pars interarticularis if someone has spondylolysis. This area is difficult to image as the pars interarticularis is blocked by multiple structures. A CT scan is able to circumvent this difficulty because of its ability to produce 3-dimensional images.

Commonly known as a CT Scan or CAT scan, this form of imaging is very similar to x-ray technology but produces many more images than an x-ray does. The multiple images produce cross-sectional views not possible with an x-ray. This allows a physician or radiologist to examine the images from many more angles than an x-ray allows. For this reason the CT scan is much more accurate in detecting spondylolysis than an x-ray. Bone scintigraphy combined with CT scan is considered the gold standard which means that it is best at detecting spondylolysis.
MRI is a newer technique used to diagnose spondylolysis and is favorable for a few reasons. The MRI is much more accurate than the x-ray and also does not use radiation. The MRI uses powerful magnets and radio frequencies to produce very detailed images of many different densities of tissue including bone and soft tissues.
Treatment for spondylosis ranges from bracing, activity restriction, extension exercises, flexion exercises and deep abdominal strengthening, that is administered throughphysical therapy. The duration of physical therapy a patient receives varies upon the severity of spondylolysis, however typically ranges from three to six months. The goal of physical therapy is to minimize movement at the unstable defect of the pars interarticularis. Once a patient completes physical therapy, and displays no symptoms or inflammation in the lower back, they are cleared to continue with daily or athletic activities. However, a patient may need to maintain a variety of rehabilitation techniques after physical therapy to prevent the recurrence of spondylolysis.
The aim of deep abdominal co-contraction exercises is to train muscles surrounding the lumbar spine which provide stability of the spine. Spondylolysis results in a spinal instability and disrupts patterns of co-recruitment between muscle synergies. Specifically, local muscles that attach directly to the spine are affected. The lumbar multifidis andtransversus abdominis play a direct role in stabilizing the lumbar spine. Instead the local muscles in individuals with spondylolysis are vulnerable to dysfunction, which results in abnormal spinal stability causing chronic low back pain. To compensate, the large torque producing global muscles are used to stabilize the spine.
Activity restriction of spondylolysis is advised for a short period of time once the patient becomes symptomatic, followed by a guided physical therapy program. Once spondylolysis has been diagnosed, treatment often consists of a short rest period of two to three days, followed by a physical therapy program. There should be restriction of heavy lifting, excessive bending, twisting and avoidance of any work, recreational activities or participation in sport that causes stress to the lumbar spine. Activity restriction can help eliminate and control a patient's symptoms so they are able to resume their normal activities. Activity restriction is most commonly used in conjunction with other rehabilitation techniques including bracing.

Acute spondylolysis is most commonly treated through the use of an anti-lordotic brace (Boston brace) to control and limit spinal movement, and reduce stress on the injured spinal segment. Bracing immobilizes the spine in a flexed position for a short period to allow healing of the bony defect in the pars interarticularis. An antilordotic brace commonly utilizes a plastic component that is contoured to closely fit the body. Antilordotic bracing subsequently reduces the athlete’s symptoms by decreasing the amount of stress on the low back, and allows a prompt return to sport for athletes. Typically, bracing is utilized for 6–12 weeks.
In order for a brace to be effective, it must be worn every day for the required amount of time. Patients are given a brace schedule determined by their physical therapist that explains the amount of time the brace must be worn daily. A brace's effectiveness increases with adherence to the bracing schedule. Patients that do not follow their bracing schedule are more likely to have their symptoms progress. Research has demonstrated that when braces are used as prescribed with full compliance, they are successful at preventing spondylolysis progression.
Most patients with spondylolysis do not require surgery but, if the symptoms are not relieved with non-surgical treatments, or when the condition progresses to high gradespondylolisthesis, then patients may require surgery. There are two main types of surgery for this condition:
Spondylolysis can have a huge impact on a young athlete's career, and may impede their future ability to perform. It is important to understand how social and psychological factors may affect rehabilitation of an injured athlete.
Frustration, anger, confusion, fear and depression are some of the psychological factors that injured athletes experience, therefore a debilitating injury can have a large impact on an athlete's mental well-being. These psychological factors can also affect recovery and return to sport as fear of re-injury often prevents athletes from adhering to rehabilitation and returning to their sport at full intensity.
Social factors can also impact the cognitive, behavioural and physical responses to injury. More specifically, social isolation from the team can have a profound psychological effect. This makes it essential to provide social support through supportive listening, emotional support, personal assistance and reality conformation.
It is also critical to educate the athletes on the rehabilitation process so they know what to expect. For instance, explaining what activities to avoid and will cause pain as well as the duration of the treatment process. In addition, it is important to select the correct treatment option for each individual. For conservative methods adherence to the exercise requires motivated patients as it can be tedious and time consuming. For instance, one study looking at deep abdominal co-contraction reported that it can take as long a 4–5 weeks to achieve this pattern of co-contraction.

